
Embryo Grading - Q&A
Written by: Jessica Manns, MBMS, BS
-
Embryos begin as one cell and are known as a fertilized egg, or zygote. This single cell is surrounded by a thick shell (zona pellucida), which surrounded the egg prior to insemination. Zygotes typically consist of 2 pronuclei (one that contains the genetic material from the egg and another that contains the genetic material from the sperm).
This single cell will undergo a process known as mitosis, or cell division. During this process, the DNA (genetic material) inside of the cell will replicate and the cell will divide into 2 cells. Each of these cells receive one copy of the DNA, so the end result is 2 cells with identical DNA. We expect to see 2 identical cells (blastomeres) in the embryo roughly 30 hours after the egg is inseminated (a sperm enters the egg). Once cell division has occurred, the embryo enters what is known as the cleavage stage.
These 2 cells will then undergo mitosis again, resulting in 4 cells with identical DNA. As the cells divide, they become smaller. However, the diameter of the embryo does not change. You can think of this like a pizza: the more slices you cut, the smaller each slice becomes. The size of the pizza does not change.
Around the 3rd day of development, an embryo should consist of around 6-10 cells, though some may consist of more cells.
On the 3rd or 4th day of development, the cells should begin to condense into a structure known as a morula (Latin for mulberry). The embryo has now completed the cleavage stage.
Later on the 4th day, a small, fluid-filled cavity (blastocoel) may begin to form within the morula. When this occurs, the embryo enters the blastocyst stage of development. At this point, the cells within the embryo begin to differentiate into 2 types:
-The inner cell mass (ICM) is a group of cells that ultimately develop into the fetus, or baby. The ICM typically looks like a round mass of cells.
-The trophectoderm (TE) cells line the shell of the embryo and ultimately develop into the placenta and other non-fetal structures.
It is difficult to tell the 2 cell types apart during the early blastocyst stage. Between the 4th and 5th day of development, the embryo should consist of roughly 100-200 identical cells. As the embryo progresses into the blastocyst stage, the ICM and TE cells become more apparent and the cavity begins to take up more space in the embryo.
Eventually, the embryo begins to expand due to the pressure from the developing cavity. At this point, the embryo increases in diameter and the shell around it begins to thin. The embryo is now known as an expanded blastocyst.
Soon after, a small hole will form in the embryo’s shell and the embryo will begin to emerge from this hole. At this point, the embryo is known as a hatching blastocyst.
And finally, the embryo will fully emerge from its shell as a hatched blastocyst. This typically occurs around the 6th or 7th day of development. An embryo must hatch from its shell in order to implant into the uterine lining (endometrium) to initiate a pregnancy.
-
It used to be common for clinics to grade embryos on day 3 of development (3 days after insemination). While some clinics still grade embryos on day 3, most clinics begin grading embryos once they reach the blastocyst stage of development on day 5.
Though embryo grading guidelines may differ between clinics, an embryo is typically graded based on its:
Stage of development (also called level of expansion)
Appearance of its inner cell mass (the group of cells that ultimately develops into the fetus)
Appearance of its trophectoderm (the cells which line the shell of the embryo that ultimately develops into the placenta and non-fetal structures)
-
Clinics often use a numeric system called the Gardner scale to record an embryo's stage of development once the embryo enters the blastocyst stage of development. The scale is from 1 to 6:
Gardner Scale 1 (early blastocyst) = once the blastocoel forms inside of the morula; takes up <50% of embryo space
Gardner Scale 2 (blastocyst) = embryo’s cells continue to divide, and blastocoel also grows in size and consumes >50% of the embryo's space
Gardner Scale 3 (full blastocyst) = once the blastocyst consumes 100% of the embryo's space
The embryo has not grown in diameter but the cells inside of it have continued to divide
It should also have a clear inner cell mass and trophectoderm at this point
Gardner Scale 4 (expanded blastocyst) = blastocoel continues expand and the embryo begins to grow in diameter and "push on" its shell (zone pellucida)
This causes the zona pellucida to begin to thin out under the pressure of the expanding embryo
Gardner Scale 5 (hatching blastocyst) = a small hole begins to form in the zona pellucida and the embryo begins to hatch from this hole
Gardner Scale 6 (fully hatched blastocyst) = embryo will then fully hatch from its zona pellucida
-
Clinics often use an alphabetical system to grade an embryo's inner cell mass (ICM) and trophectoderm (TE). While many clinics use an A-C scale, others use an A-D scale.
Inner cell masses are typically graded as follows:
A = present, compact, many cells, above average
B = present, fairly compact, average number of cells
C = present, not compact, fewer cells than average
D = not present or degenerate
Trophectoderms are typically graded as follows:
A = many cells, uniform in appearance, no gaps, above average
B = many cells, mostly uniform in appearance, small gaps, average
C = few cells, many gaps, not uniform in appearance, below average
D = no cells or degenerate
While "D" quality embryos are often not recommended for transfer, "C" quality embryos can be transferred and result in healthy live births. However, the poorer an embryo's grade, the lower its chance of success.
-
Keep in mind that embryo grading is subjective, meaning that it can vary from person to person. And, again, each clinic may have its own grading system.
If your clinic's grading system differs from the system described above, reach out to your clinic for an explanation of its grading system.
Embryo grading cannot determine if the embryo has genetic or other underlying abnormalities.
While high quality embryos have higher success rates than low quality embryos, they cannot guarantee a successful outcome..
Poor quality embryos have the ability to result in healthy live births, though their success rates are lower than high quality embryos.
Picture Examples

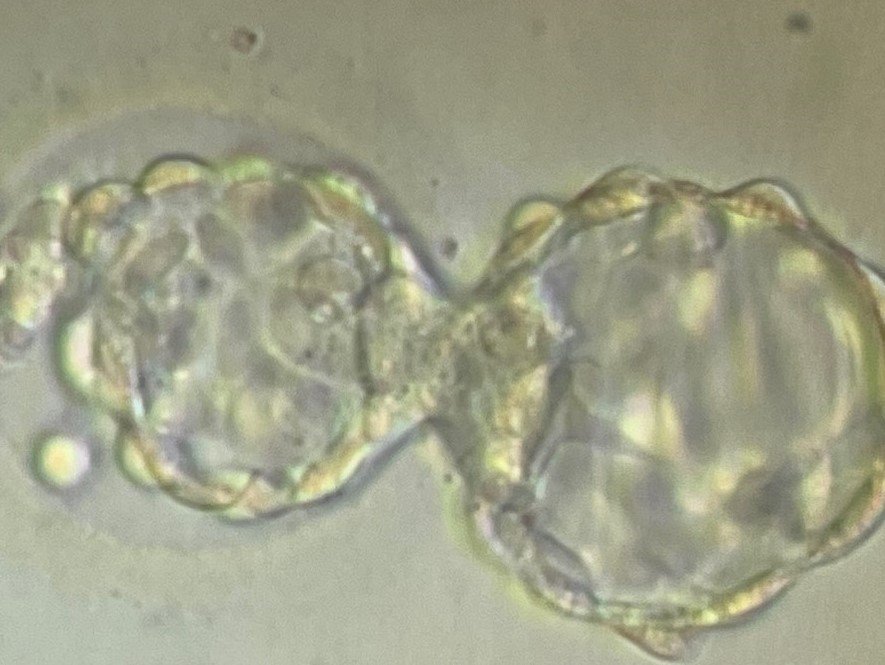
Left Image: this embryo is expanded (its zona pellucida is thin but it isn't hatching yet). It has a fairly compact inner cell mass in the 6 o clock position. The trophectoderm is present but not completely uniform and it has some gaps at the top. This embryo would be graded as a 4BB.
Right Image: this is a hatching embryo with a compact inner cell mass and above average trophectoderm. This embryo would be graded as a 5AA.